Cette traduction automatisée est fournie à titre informatif et peut contenir des imprécisions. La version originale est disponible via le bouton de téléchargement ci-dessous.

The role of ozone therapy in maintaining the articular function and in relieving the pain for patients with knee osteoarthritis
2 Balneary Sanatorium „Vraja Marii” Eforie South - Constanţa
ABSTRACT
Ozone Therapy is thought to be a non-pharmacological therapy, which makes use of oxygen and ozone, It is based on the ozone characteristics, such as the antibacterial and antimycotic, anti-inflammatory and immunomodulatory, of systemic modulation of homeostasy and of the optimization of the way the organs and systems function, but also of tissue bionourishing. Some of the beneficial effects of the ozone are: the enhancement of the oxygen supply in the tissues affected by inflammation and pain, the increase of the blood stream and the removal of the metabolic waste in the joints affected, the obstruction of the substances which maintain the inflammation and pain, an immunomodulatory action upon the whole body, the stimulation of the health improving mechanisms in the body, a mio-relaxing action and thus, a better joint mobility and a better body system functioning.
Keywords: ozone therapy, knee osteoarthritis, physiotherapy.
Objectives
The present study was aimed at showing the evolution of the pain and of the body system functioning in knee osteoarthritis for patients who were given ozone therapy only, compared to the patients who followed the physio-kineto therapy in the Balneary Sanatorium “Vraja Marii” in Eforie South.
Taking into account that the physio-kineto treatment is contra-indicated or restricted to patients with chronical rheumatologic diseases and who, in many cases, show associated cardio-vascular pathology (high blood pressure, coronary disease, AVC after-effects, etc.), ozone therapy can be an efficient alternative.
Introduction
Dr. Iliescu M.
Department of Anatomy, Faculty of medicine, University “Ovidius” Constanţa, Romania
Aleea Universitatii, Nr. 1, Campus B
Constanţa, Romania
madalina@anatomie.ro
25
This was a prospective study, run over a period of five yearsfrom 1 July 2016 to 30 June 2021 in Yalgado OuedraogoTeaching Hospital neurosurgery department in Ouagadougou,Burkina Faso.
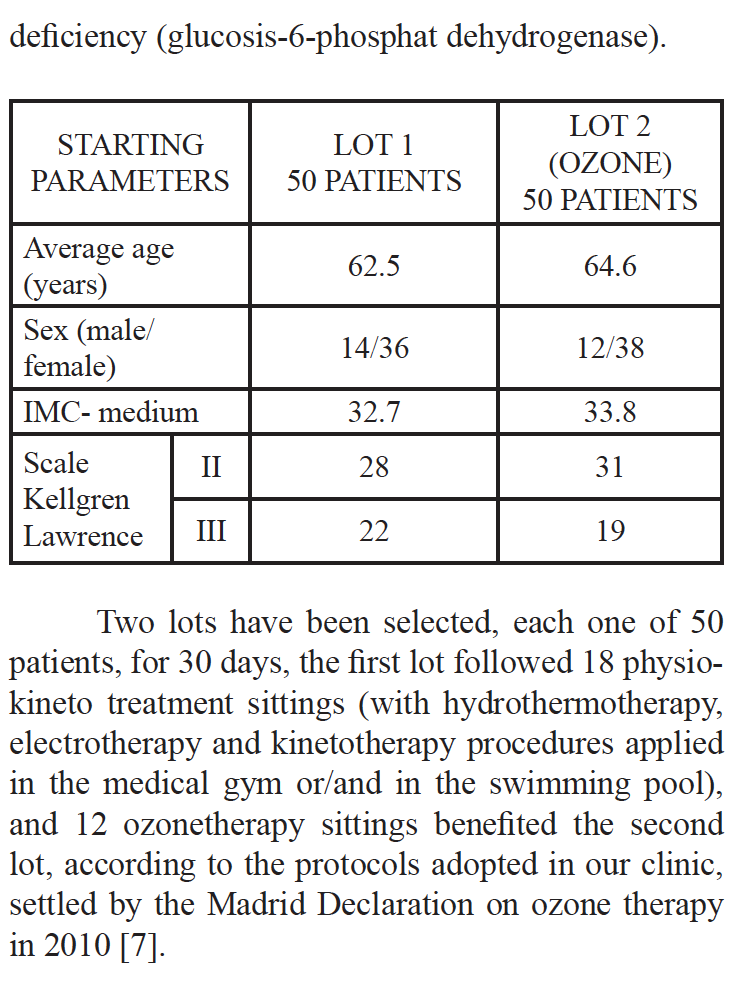
Two lots have been selected, each one of 50patients, for 30 days, the first lot followed 18 physiokinetotreatment sittings (with hydrothermotherapy,electrotherapy and kinetotherapy procedures appliedin the medical gym or/and in the swimming pool),and 12 ozonetherapy sittings benefited the secondlot, according to the protocols adopted in our clinic,settled by the Madrid Declaration on ozone therapyin 2010 [7].
Material and Method
The present study was carried out in the period between 01.07.2012 and 15.12.2012, within the Balneary Sanatorium “Vraja Marii “ Eforie South.
There have been included in the study 100 patients with clinical symptomatology of primary bilateral knee osteoarthritis, diagnosed according to the criteria of the American College of Rheumatology, with radiological modifications on Kellgren-Lawrence (II-III) scale, with quantified values of the pain on the visual analogue scale VAS between 4 and 7, with functional result effected by filling in the questionnaire WOMAC, patients aged between 50 and 65 years old, with the average duration of the disease longer than 12 months.
There have not been included the patients with secondary gonarthrosis (gout, rheumatoid polyarthritis, psoriasis arthritis, TBC arthritis, etc.). When patients were selected to be treated with ozonetherapy, the contraindications were taken into account (hyperthyroidism, trombocytopenia, pregnancy, recent myocardial heart attack, G-6:PD-
Work technique
The recovery-rehabilitation program of the patients had the following general points: decreasing the pain and the inflammation, maintaining or increasing the muscular force and the joint mobility, the amelioration of life quality and the prevention of the disfunctionalities and invalidity.
As methods of physio-kineto treatment, we have used procedures of hydrothermotherapy, mud and paraffin packing, mud baths, plant baths, bubble baths, underwater shower, aimed at sedating and releasing the compression on the nerve root structures; we also used the antalgic electrotherapy and that of stimulating the muscle system at the risk of atrophy (quadriceps); kinetotherapeutical techniques in the gym or in the pool with water from Techirghiol Lake
To the patient with his knee in a slight flexion position, one prefers the painful places and the tendon inserting zones at the pes anserinus and iliotibial levels.
We used the medical ozone OM302 generating device. Special attention was paid to an accurate control of the ozone supply concentrations and of the right quantity given to the patients.
The adjustment and the measurement are done in due time; when a concentration index is adjusted., the generator produces ozone and measures the concentration programmed and done until it reaches the index selected, all this followed by an action of a catalyzer which neutralizes (absorbs) the additional ozone. In practice we used doses of 2-5 μg/ml, 40-50 ml 03.
Several infiltrations at the knee level are given, in doses of maximum 5 ml on injection point [8,9]. At the end of the infiltrations the patient is invited to move several times in successive flexion/extension motions for a better distribution of the gas at the level of articulation and also at the level of recurrences In all were 12 treatment sessions for each patient.
The evaluation of the patients was done on the first day and after 4 weeks by means of index score of the arthrosis (Western Ontaris and MC Master Universities Osteoarthritis Index- WOMAC) and of the visual analogue scale for pain assessment in passive and active motion (Visual Analog Scale - VAS). Other parameters have also been evaluated such as length of time taken when climbing down 20 steps in normal walking, before and after the treatment, as well as mobility in the knee joint (in degrees) on flexion movement.
The WOMAC questionnaire of evaluating the patients suffering from gonarthrosis includes a set of 24 questions filled in exclusively by the patient, without the assessor’s interference. The index score is based on maximum 96 points and it is made up of 3 sections: the first one (A) with 5 questions evaluates the pain, the second one (B) with 2 questions, indicates the mobility and the 3rd section (C), with 17 questions, showed the functional level.
The patient will point to one of the following choices: absent, slight, moderate, severe and extreme. He is asked to read the question carefully and to make the right choice, depending on his condition. The average time duration necessary for filling in the questionnaire is of about 15’.
After the questionnaire has been filled in, the assessor sums up the points, in this way: absent = 0 points; slight = 1 point; moderate = 2 points; severe = 3 points; extreme = 4 points.
A large number of points at the score WOMAC presents an unsatisfactory result. Thus:
z > 38 points = unsatisfactory
z 29-38 points = acceptable
z 15-28 points = good
z 0-14 points = excellent
The visual analogue scale used (VAS)
includes a scale of 100 mm, with two marking points (0 for absence of pain and 100 for the pain at the highest possible degree of endurance)
0 --------------------------------------------- 100 without pain the worst possible pain
In our case, the patient marks a point between the two indices, according to his own perception of the pain felt in passive and active positions of the knee,
As a result of the patients evaluation at the moment of their hospitalization and after a period of 4 weeks they were distributed into two study lots, according to the pre-settled parameters (WOMAC scale, VAS scale, time and degree of mobility), data whose interpretation lead to the following conclusions.
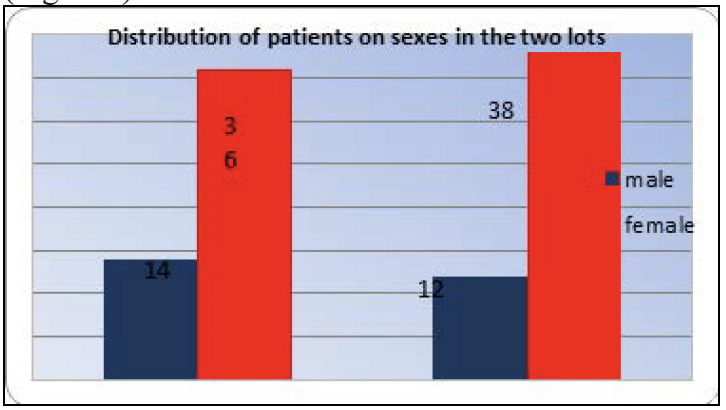
When distributing the patients on sexes, one can notice the prevalence of the females in both lots (Figure I)
During the evaluation period, there wasrecorded a favorable evolution of the pain on VASscale, both in the lot I and in the ozonetherapy lot,more noticeable to patients who was applied thephysio therapy treatment. We notice that mostpatients suffering from arthrosis feel considerableamelioration of the pain when actively moved theknee joint (Figure II).
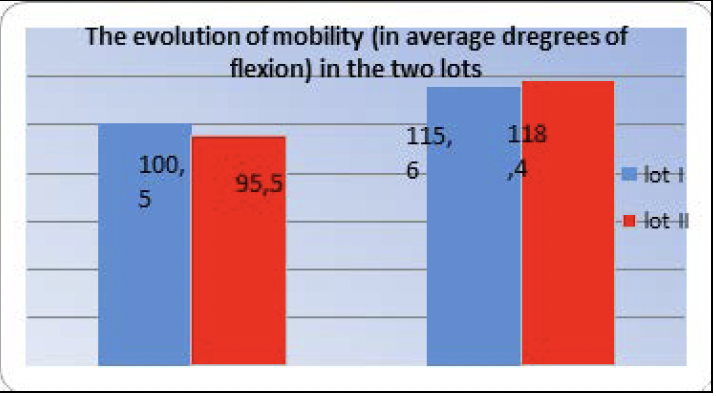
as a result of the goniometrical measurement at the level of each group, with a slight prevalence in lot 2 (Figure III).
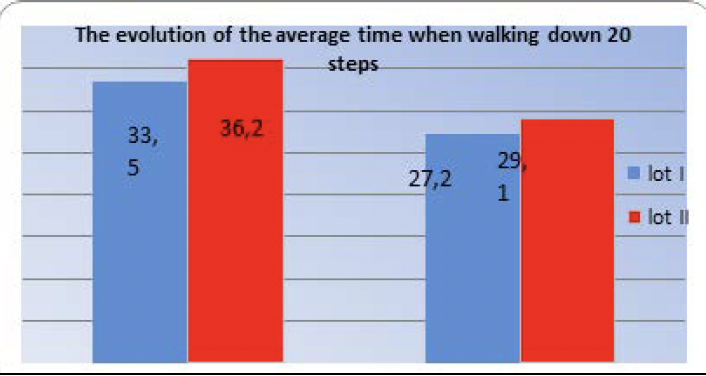
Also, the average time when walking down20 steps shorted in both groups, but without anynoticeable differences from a statistical point of view(Figure IV).
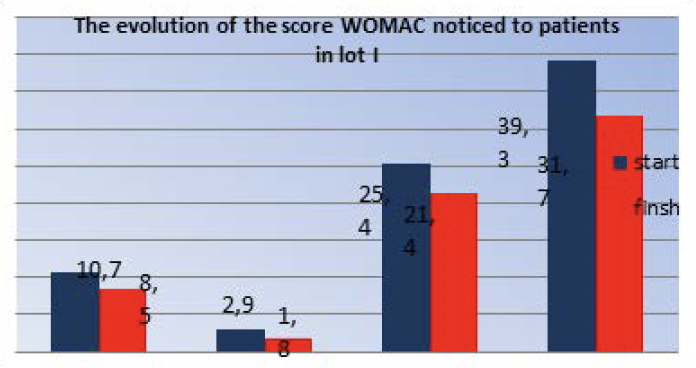
When analyzing the parameters of the WOMACscore, the following ideas have been noticed:In lot I there was a decrease of the wholescore from unsatisfactory values (indices - 39.3) toacceptable values (31.7) (Figure V).
The group II had an evolution of the WOMACscore from acceptable values (indices - 35.6) to goodvalues (indices - 22.9) (Figure VI).

Conclusions
Both physical and kinetic therapy and ozone therapy are efficient in reducing the pain, proven by the WOMAC score for patients with knee osteoarthritis, having radiological score Kellgren-Lawrence ≥ 2, with a visual analogue scale of pain ≥ 4 and with unsatisfactory response to the therapy with nonsteroid and condroprotective anti-inflammatory drugs. The ozone therapy, even when used as the only therapy, brings further benefits, considerably relieving the pain and the WOMAC score and having a high impact upon the functional systems and quality of life. It also shows a major advantage for the patients with contraindications for physiotherapy, it is a low invasive procedure, well tolerated by the patient and with considerably low costs related to its results.
References
1. Bocci V. (2005). OZONE - A New Medical Drug. Dordrecht, Netherlands: Ed. Springer
2. Bocci V. (2002). Oxygen-ozone Therapy - A Critical Evaluation. Dordrecht, Netherlands: Kluwer Academic Publishers
3. Bocci V., Zanardi I. & Travagli V. (2010). Potentiality of oxygen-ozone therapy to improve the health of aging people. Curr Aging Sci. 3:177-187
4. Calungaa J.L., Menéndeza S., León R., Chang S., Guanche D., Balbín A., Zayas J. & García P.(2012). Application of Ozone Therapy in Patients with Knee Osteoarthritis. Ozone: Science & Engineering: The Journal of the International Ozone Association. 34(6), 469-475
5. Benvenuti P. (2006). Oxygen-ozone treatment of the knee, shoulder and hip. A personal experience. Rivista italiana di ossigeno-ozonoterapia. 5,
135- 144
6. Bocci V. (2006). Scientific and Medical Aspects of Ozone Therapy. State of the Art. Archives of Medical Research. 37(4), 425 - 435
7. Royal Academy of Medicine in Madrid, Spanish Association of Medical Professionals in Ozone Therapy. (2010). International Meeting of Ozone Therapy Schools 2010. Madrid, Spain
8. Genovese E., Bonetti M. & Fontana A. et Al.(2004). Tecnica della infiltrazione guidata di ossigeno-ozono nelle principali articolazioni. Rivista Italiana di Ossigeno-Ozonoterapia. 3, 121 - 130
9. Ikonomidis St., Charalambus D., L. Vakirtzian
L. & Iliakis E. (2002). Non Operative Treatment of Shoulder Impingement Syndromewith Topical Injections of Medical Oxigen-Ozone Misture. A Double Blind Clinical Trial. Rivista Italiana di Ossigeno-Ozonoterapia. 1, 41 - 44