Cette traduction automatisée est fournie à titre informatif et peut contenir des imprécisions. La version originale est disponible via le bouton de téléchargement ci-dessous.


To cite this version:
Original Article
Purpose: To assess safety and effectiveness of computed tomography (CT)-guided intradiscal oxygen-ozonetherapy (O2-O3 therapy) for the treatment of symptomatic lumbar disc herniation and radiological changes.Materials and Methods: This study was conducted in twenty patients presenting lumbar disc herniation withresistant lumbar or lumbar radicular pain They underwent intradiscal oxygen-ozone therapy under CT guidance.They were treated at one- or two-disc levels, representing a total of 24 discs treated. MR imagingexaminations were obtained before treatment and 2 months post-procedure to analyse treatment-relateddisc modifications including modification of the surfaces of the disc and of the herniated disc, and the variationsin disc height according to the disc height index. Clinical outcomes were assessed using the visual analoguescale (VAS) to evaluate the severity of pain before the procedure, at primary (2 months) and atsecondary (12 months) follow-ups.Results: All the procedures were technically successful. The median VAS scores were 7.95 before the procedure,3.9 at 2 months and 2.95 at 12 months. MRI analysis showed a significant decrease in herniation size at2 months (-20%, p = 0.008). No immediate or late complications were observed. Only three patients (13.6%)underwent lumbar spine microdiscectomy in the year following ozone therapy. The treatment appeared tobe more effective in cases of nerve root symptomatology.Conclusion: This study suggests that intradiscal O2-O3 therapy is safe and effective for the treatment of lumbardisc herniation associated with resistant lumbar or lumbar radicular pain.
1. Introduction
Nonspecific nerve root pain and low back pain are two of the mostcommon cause of disability in the world. More than three out of fourpeople will experience several episodes of lumbar and/or radicularpain during their lifetime.1Most of the time, the pain disappears spontaneously or after conservativetreatment. Otherwise, it becomes a real public health
* Corresponding author at: Daphne GUENOUN, MD PhD, APHM, Sainte-MargueriteHospital, Institute for Locomotion, Department of Radiology, 270 boulevard sainteMarguerite 13009 Marseille, France.E-mail addresses: clementine.simon@ap-hm.fr (C. Simon), Thomas.lecorroller@aphm.fr (T.L. Corroller), Vanessa.pauly@ap-hm.fr (V. Pauly), Maud.creze@aphp.fr(M. Creze), Pierre.champsaur@ap-hm.fr (P. Champsaur), Daphne.guenoun@ap-hm.fr (D.Guenoun).
problem with social and economic impacts. Therapeutic planning traditionallybegins with noninvasive treatment based on pharmacologicaland rehabilitation treatments. If conservative treatment,including rest, medications, and physical therapy, failed to relieve thepain, facet joint or epidural corticosteroid injection is considered(periradicular corticosteroid injection is not recommended in Francebecause of its potential side effects).When this treatment is not sufficiently effective, minimallyinvasive percutaneous techniques including intradiscal steroid,chemonucleosis, intradiscal decompression, laser, discectomy, andannuloplasty, are an interesting alternative to avoid or delay surgicaltreatment.2,3Intra-discal O2-O3 therapy is a minimally invasive and inexpensiveprocedure feasible under CT-scan or fluoroscopic guidance. Thetreatment principle is based on reducing the volume of the disc and
the pressure on the adjacent nerve root, without affecting spinalcanal.4The use of ozone (O2-O3 therapy), the tri-atomic form of oxygen,has many advantages, including its low cost, ease of manufacture andsafety for adjacent structures, with few complications.4,5Ozone injection induces an oxidation reaction. By oxidizing theproteoglycans contained in the disc nucleus, ozone is responsible fordehydration, with a reduction of the disc volume and pressure and aresorption of hernia. Its chemical properties are anti-inflammatoryand anti-nociceptive. Despite its low cost, the ease of the techniqueand the good results reported in the literature, intra-discal oxygenozonetreatment is not wildely used in France. Because intra-discalO2-O3 therapy is not well known to clinicians and radiologists, only 3cities all over France offer this treatment.Previous studies have shown the clinical efficacy of intradiscalozone therapy in low back pain and nerve root pain caused by lumbardisc herniation (LDH) but there is no consensus on the selection ofpatients, nor on the injection method: fluoroscopic or CT-guidance,general or local analgesia, total gas volume, ozone concentration, frequencyof injection, use of periforaminal steroid and local anesthetics.Your experience could be considered to constitute a contribution toan effort to validate this technique.The main objective of our study was to assess the effectivenessand safety of intradiscal O2-O3 therapy. The second objective was toanalyse radiological changes and criteria for good therapeuticresponse.
2. Materials and methods
2.1. Study design
We started intradiscal O2-O3 therapy in our centre in 2018, underCT-guidance, and we followed the first twenty-two patients treatedwith ozone during the first-year post-treatment.Institutional review board approval was obtained for this studywith waiver of written informed consent for the review of clinicaland imaging data.
2.2. Inclusion and exclusion criteria
We included patients (from 20 to 85 years old) treated by oxygenozonetherapy at one or more disc levels, at Sainte Marguerite Hospital,APHM, Marseille, France between 2018 and 2019.
Inclusion criteria were as follows: patients suffering from lowback pain and/or radicular leg pain; persistent pain for at least 6months that was nonresponsive to conservative treatments; at leastone epidural or facet joint corticosteroid injection in the last pastyear without pain relief or with an improvement in pain of less than2 months. Lumbar protrusion level discopathy on MRI correspondingto the level of pain. No interventional pain treatment was appliedwithin the last 3 months and patients needed a pain score equal orgreater than 4 on the visual analogic scale (VAS).
The mean time to complete the procedure was approximately25 min.The patient was kept for overnight observation and dischargedthe next morning. Return to work was permitted 7 days after the procedure.2.4. Outcome measures2.4.1. Clinical dataFirst consultation was performed one month prior to the procedure,the second consultation (including MRI) between 5 and 12weeks after the procedure (on average 8 weeks) and the third consultationwas conducted between 11 and 15 months after the procedure(on average 13 months).At each consultation, patients were evaluated for pain using thevisual analogue scale (VAS). The patient’s age, gender, initial symptomatology(lumbar, root or mixed pain) and a history of epiduraland/or posterior joint corticosteroid infiltration, other minimallyinvasive methods or lumbar surgery were noted at the initial consultation.During the first consultation we identified radiological disc anomalies,such as a herniated disc, that may explain low back pain with orwithout root pain, to select patients eligible for the procedure. Thenwe informed them of the principles of the treatment and explain thebenefits sought and the risks (e.g., haematoma, infection, compression).The treatment was considered effective if there was a decreasein the VAS score greater than or equal to 3 points at the 2-month consultation.At the one-year consultation, the patients completed the modifiedMacNab questionnaire (Appendix 1) to assess the effectiveness of thetreatment.72.4.2. Radiological dataTwo MRI examinations were performed, first, prior to the procedure(less than one month before procedure), and second from 2months after procedure. No additional MRI was performed at the 12months follow-up.The MRIs were performed on 1.5 or 1 T devices (PHILIPS Achieva1,5T 2004, PHILIPS Ingenia 1,5 T omega 2015, PHILIPS Panorama HFO1T 2013) with usual spine sequences (sagittal T1-, T2-, STIRweightedimages, and axial T2 weighted).Two radiologists, a junior with 4 years of experience (CS) and asenior with 10 years of experience (DG) reviewed the initial and 2-month follow-up MRI images in consensus. They were blinded to theinitial pre-procedure MRI.We analysed the following criteria:− The modification of the surfaces of the disc and of the herniateddisc: in the axial plane, we contoured the disc with the ROI (regionof interest) tool to obtain its surface. We did the same for the hernia.− The variations in disc height according to the disc height index(DHI)8− The following initial radiological characteristics: The type of disc herniation: bulging, protrusion, extrusion The location of disc herniation: postero-median, postero-lateral,foraminal, extra-foraminal The contact or compression on the nerve root The endplate changes according to the Modic classification9 The severity of disc degeneration according to the Pfirrmann’sclassification10 The presence or absence of calcifications in the disc herniation The presence of a high-intensity zone (HIZ) defined as highintensitysignal located in the substance of the posterior annulusfibrosus.11
Exclusion criteria were as follows: patients with motor deficits,systemic infection, coagulation disorders, pregnancy, VAS pain scorelower than 4, no pre-procedure MRI, and those who did not benefitfrom follow-up consultations.2.3. Procedural techniqueIntravenous analgesia was administered during the procedure(paracetamol 1 g § tramadol), and MEOPA (nitrogen monoxide-oxygenmixture) was given if necessary.The procedure was completed under strictly sterile conditions(without prophylactic antibiotics6) under computed tomographicguidance (CT GE light speed 2009 classe 3).The patient was positioned in ventral decubitus in the CT-scanroom. After local anaesthesia (Lidocaine 2% 5 ml), a posterior-lateralapproach was employed. The side of approach corresponded to theside of maximal pain as described by the patient.The ozone-oxygen mixture was produced in real time by amedical ozone generator (Ozo2futura; Alnitec). High-pressurepure medical oxygen cylinders were used to transform O2 in O3,and a Millipore bacteriological filter was placed between thesyringe and the generator.When the tip of the needle (Orgapix, size 22 gauges, 20 cm)reached the centre of the nucleus pulposus, 4−7 ml of gas mixture(30 micrograms/ml concentration) was injected (Fig. 1).A CT scan confirmed the diffusion of gas into the disc and the herniation.No corticosteroids or local anaesthetic were injected into the discor epidural space during the procedure.The mean time to complete the procedure was approximately25 min.The patient was kept for overnight observation and dischargedthe next morning. Return to work was permitted. Theozone-oxygen mixture was produced in real time by a medicalozone generator (Ozo2futura; Alnitec). High-pressure pure medicaloxygen cylinders were used to transform O2 in O3, and aMillipore bacteriological filter was placed between the syringeand the generator.When the tip of the needle (Orgapix, size 22 gauges, 20 cm)reached the centre of the nucleus pulposus, 4−7 ml of gas mixture(30 micrograms/ml concentration) was injected (Fig. 1).A CT scan confirmed the diffusion of gas into the disc and the herniation.
2.5. Statistical analysis
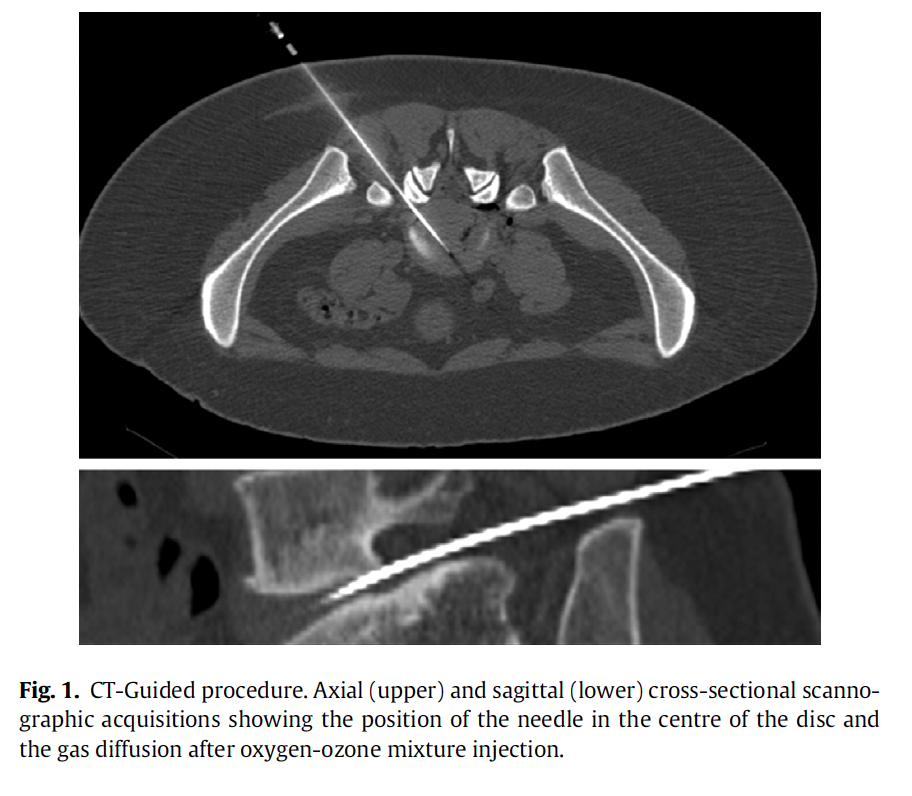
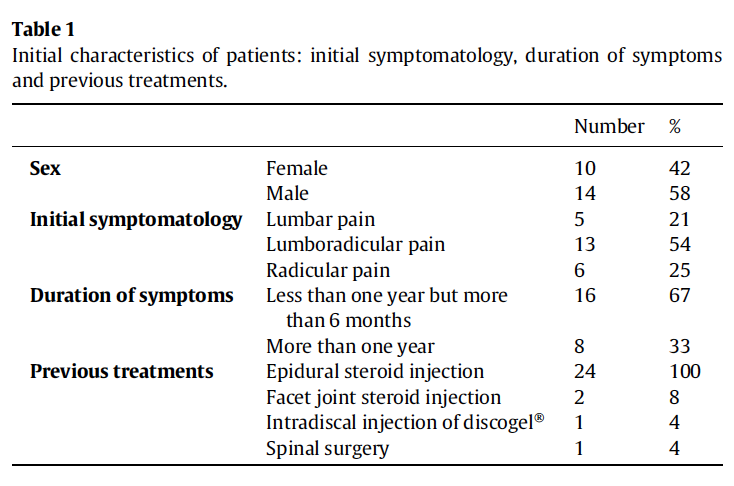
First, we described the population included using means and standarddeviations (or medians and interquartile ranges) for quantitativedata and using numbers and percentages for qualitative data.Then, we compared subjects whose decrease was greater than orequal to 3 points at 2 months with other subjects by performing univariatestatistical analyses: chi-square or Fisher’s exact test for percentagecomparisons and means (or nonparametric) Mann-WhitneyU tests for quantitative variables. Statistical significance was maintainedat the alpha threshold of 5%. Statistical analyses were performedwith SPSS V20 software.3. Results3.1. Description of the populationBetween 2018 and 2019, 22 patients received intradiscal oxygenozonetherapy, with a total of 27 injections.We excluded a man and a woman (the first had two discs levelstreated at the same time) because they did not participate in the secondand the third consultations.In total, 20 patients, 12 men and 8 women aged 26 to 80 years(mean age = 47 years), were included, representing 24 injections:two patients were treated at 2 levels at the same time, 2 patients at 2levels at 1-year intervals.All patients received epidural steroid injection (Hydrocortancyl2.5%) in the last past year. 10 patients had no pain improvement. The10 other patients had an improvement between 2 days and 2 months(mean= 3 weeks).Table 1 shows the initial clinical characteristics of the patients.Most of them had been in pain for less than a year (but more than sixmonths). The most frequently treated levels were L4-L5 (N = 9) andL5-S1 (N = 11), followed equally by L2-L3 (N = 2) and L3-L4 (N = 2).3.2. Clinical resultsThe mean VAS score before the procedure was 7.95. The meanVAS score was 3.9 at two months and 2.95 at one year.On average, VAS scores decreased by 4 points at two months andby 4.9 points at one year (p<0,0001) (Fig. 2).A decrease of 3 points or more was observed in 81.8% of patientsat 2 months and 86.3% of patients at 12 months.No complications related to intradiscal injection of oxygen-ozoneinjection were identified, sooner or later (up to one year). Sometimes,during the injection, we could see a leak of O2-O3 in the epiduralveins, without clinical impact.In the twenty patients included in the study, the success rate,according to the modified MacNab criteria was 65%, with 20% (N = 4)
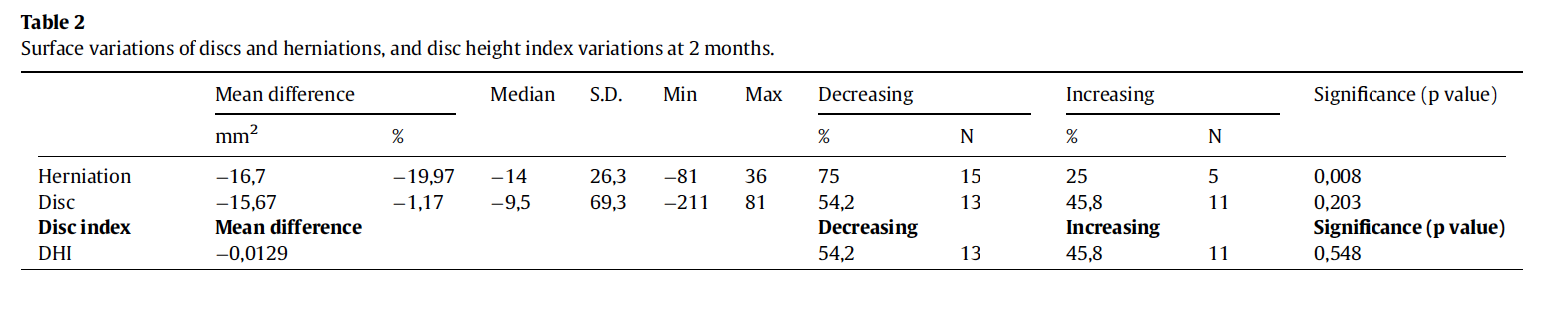
excellent responses, 25% (N = 5) good responses and 20% (N = 4) satisfactoryresponses. The failure rate of 35% was mainly due to 30% poorresponses (N = 6), and to 5% incorrect response rate (N = 1). amongstthe failure of the treatment, the surgery rate was 15% at one year,representing 3 patients at 4, 6 and 11 months respectively after theprocedure. These patients had lumbar radicular pain (N = 2) andradicular pain (N = 1), respectively.No perioperative difficulties were reported by the surgeons. Noadhesions between soft tissue and bone structures were unexpectedlydiscovered, contrary to what was reported in the study by Vanniet al. after intraforaminal ozone injections.123.3. Radiological resultsAt two months, herniation disc surfaces decreased significantly in75% of cases: the mean reduction was approximately 20% (Table 2,Fig. 3).Disc surfaces and disc height, according to the DHI, tended todecrease, but without statistical significance (Table 2).
3.4. Correlations with treatment effectiveness
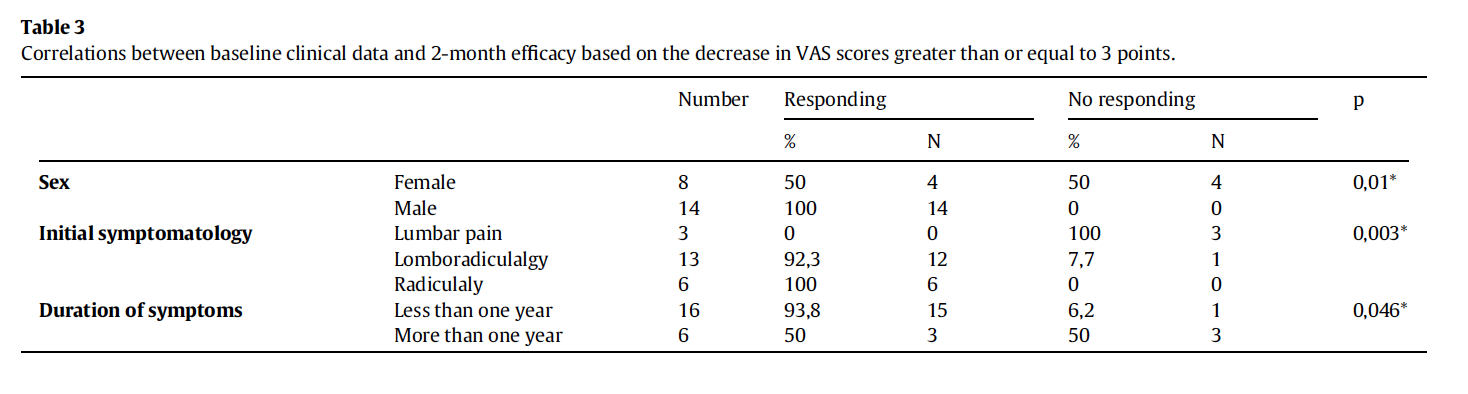
We found significant correlations between clinical efficacy andsex, initial type of symptomatology and initial duration of symptoms(Table 3).Indeed, all men (100%) had a significant improvement in paincompared to only half of women (50%).Treatment was more effective in patients with radicular pain:100% for isolated radicular pain, 92.3% for mixed lumbar and radicularpain, and 0% for isolated low back pain (p = 0,003).

Finally, treatment was more effective if the pain lasted less thanone year (100%) than if it lasted more than one year (50%) (p = 0,046).We found no significant differences by age or initial radiologicalparameters (Table 3).According to the modified MacNab criteria, intra-discal O2-O3therapy was successful for all the patients with extra-foraminal(N = 2) and median hernia (N = 1), for 2 of the 3 patients who had aforaminal hernia, and for 8 of the 14 patients who had a postero-lateralhernia.However, we noted that all patients with calcified disc herniationresponded well to the treatment (100% versus 77,8% if there were nocalcifications in the herniated disc, p = 0,99). We did not find any significantcorrelation between pain improvement and the reduction indisc surfaces or disc height.
4. Discussion
4.1. Clinical efficiency
The natural history of disc herniation symptoms is to disappearover time. However, for some patients, the pain is too intense and/or
too prolonged, and more radical treatments can quickly improve thesituation.As we have shown in our study, oxygen-ozone therapy can acceleratethe healing process in these patients, with a significant and prolongeddecrease in the VAS scores at 2 months and even more at 12months.The efficiency of oxygen-ozone therapy has already been demonstratedby other studies, with a reduction of the VAS score in 62 to93% of cases (mean 3.9 points).13,1465% of patients treated with oxygen-ozone had a successful outcomeat one year follow-up, according to their McNab clinical outcomescores. This result compares favourably to studies assessingintra-discal ozone: Steppan et al.13 found in a metaanalysis a successrate of 79% (for all follow up dates) and Crockett et al.15 found a successrate at 68% at 6 months. Despite these encouraging results, inthe literature and to date the intradiscal procedures are not recommendeduntil rigorous controlled trials prove their efficacy.Unlike most studies, we did not conduct concomitant epidural orforaminal injections of corticosteroids because all patients receivedtreatment by corticosteroid infiltration with treatment failure. In themetaanalysis of Steppan et al.,13 in 9 out of 12 studies, intra-discaloxygen-ozone treatment was associated with a periradicular corticosteroidinjection. Ezeldin and al.16 added a periradicular injection ofthe same O2-O3 mixture, steroid, and local anaesthetic. Therefore, inthose studies, it is difficult to know if the clinical efficacy comes fromozone treatment or corticosteroid treatment. The study of Ercaliket al.16 is the only study that compares intra-discal O2-O3 therapyalone versus intra-discal O2-O3 therapy with periforaminal steroidinjection. This randomized study demonstrated that intradiscal ozoneinjection alone was sufficient to treat low back pain and leg paincaused by LDH, and that periforaminal steroid injection does not provideadditional benefit.MacNab qualitative scale was designed to assess functionalimprovement. The subjectivity of the criteria constituting the modifiedMacNab scale as well as the lack of precision of the questionsand answers may have been a limitation of our work. However, Mac-Nab scale has been widely used in other studies in evaluation ofpatients’ pain response and disability.5Three patients underwent surgery. For one of them, the oxygenozonetreatment had been temporarily efficient. For another, symptomsimprovement was insufficient and for the last one, no pain reliefwas noticed. For this third patient, surgery remained ineffective. Thisrate was also found in other oxygen-ozone therapy studies (18%)13and is similar to intradiscal laser (4.4−25%),17 nucleoplasty (18.7%),18and chymopapain (5−30%)19 treatments. Therefore, oxygen-ozonetherapy does not appear to be inferior to other minimally invasivemethods.This low rate seems acceptable, given the number of surgeriespotentially avoided. Furthermore, intradiscal oxygen-ozone treatmentprocedure last 25 min and the price is very low compared tosurgery. Finally, ozone does not preclude recourse to traditional surgeryif it should fail. Indeed, the surgeons who took charge of the 3patients did not report any difficulty during the surgery: they did not
find any adhesions between the soft tissues and bony structures, contraryto the article of Vanni et al.12 No side effects were recorded ateither short- or long-term follow-up (until one year). In the literature,the complication rate reaches 0,6%.13Most complications are minor and transientl. They consist of vagaldiscomfort during the procedure. We did not face this problem, probablybecause we slowly injected small volumes of gas and used subcutaneousanalgesia.The predominant serious complications described were infectiousand more frequent at cervical stage.20-22 Ozone is a powerful oxidantand an excellent disinfectant. Antibiotic prophylaxis does not seemessential at the lumbar level6 and strict asepsis is sufficient.Furthermore, the CT-guided injection allows to monitor the gasdiffusion, and thus to avoid certain complications.
4.2. Radiological modifications
Disc-size reduction was not statistically significant in our study. Inthe literature, however, this result is quite unanimous,23-26 probablyrelated to the dehydration properties of ozone on the disc. Nevertheless,the reduction does not seem to be significant until the 6thmonth.27Our early control (at two months) and our small number ofpatients may explain the lack of significant results.However, most studies, such as ours, have found a significant sizereduction of discs herniation (DH),17,28 except the study by Apuzzoet al.,29 who found herniation size reduction in only 36% of cases.Ozone, therefore, seems to have an effect first on disc herniation,probably by decreasing disc pressure with a reabsorption effect, andthen on the entire disc in relation to disc dehydration. But even ifdisc herniation has persisted in patients for several months or yearsbefore oxygen-ozone therapy, it cannot be excluded that thedecreased size of disc herniation wasn’t due to the natural progressionof disc herniation.
4.3. Correlations with efficiency
To compare the effectiveness of the treatment, according to theclinical and radiological parameters, we created 2 groups: theresponding group if the VAS scores decreased by 3 points or more at2 months and the nonresponding group if the scores decreased byfewer than 3 points. This three-point threshold seems to correspondto adequate pain control.30We found better efficiency on root symptoms, with or withoutlow back pain, and resistance in the case of isolated low back pain.Although it is recognized that radicular pain is a better clinicalindication for O2-O3 therapy than low back pain,31,32 to our knowledge,no study has proven it to date.Given these results, we wonder whether this treatment is usefulin cases of isolated low back pain. The systematic review of Costaet al.5 confirm that little evidence is available on the effect of ozoneinjections in patient with low back pain due to lumbar disc herniation.Indeed, most low back pain is non-specific, and in case of
isolated low back pain, several lumbar structures are plausible sourcesof pain (eg, the intervertebral disc, the facet joints, the vertebralendplates), but clinical tests do not reliably attribute the pain to thosestructures.Bryce et al. also found lower efficacy in women.33 They usedanother minimally invasive therapy, electrothermal intradiscal therapy(IDET). We believe that independent parameters, such as psychologicalfactors, and that more comprehensive management of painshould be implemented in women.34-36The finding of better efficacy in our study if pain lasted from lessthan one year was discordant with the findings of Bonetti et al.24:they showed that oxygen-ozone treatment remains effective whenthe pain was evolving for more than 2 years.We did not find a significant correlation between the initial radiologicalparameters, including the changes in disc and herniationsizes.Treatment was no more effective in mild and moderate discdegeneration than in severe disc degeneration, contrary to the findingsof Perri et al.37No other studies have examined the issue of effectiveness in relationto Modic changes. For the other results, the previous studieswere variable.Muto et al.38 did not find a correlation between disc-size reductionafter oxygen-ozone nucleolysis and pain reduction, but Elawamyet al.25 found a significant correlation between the percentage reductionin DH and the decrease in the VAS score.Perri et al.37 showed that extrusion and protrusion disc herniationshad a better response than bulging disc herniations, but thisresult was contradictory to what Ghatge et al.’s study.39 Amorettiet al.40 was the only study that found that treatment was more effectiveif the disc herniation was posterolateral or foraminal than if itwas posteromedian.Moreover, several studies have shown that the presence of calcificationsin the herniated discs was predictive of failure.38,41In our study, treatment was successful for the 4 patients with calcifieddisc herniation. These studies did not specify whether the herniateddiscs were very or slightly calcified and, in our series, theywere very poorly calcified.The association of ductal stenosis was identified as a potential biasby Lu et al.41In any case, the presence of small calcifications in the herniateddisc should not be considered as a treatment resistance factor.4.4. Strengths and limitations4.4.1. StrengthsIn our study, patients were representative of the population thatwas eligible for this procedure. The inclusion criteria were broad,including patients ranging from 26 to 80 years in age with all types ofdisc herniations.The patients benefited from the same protocol undertaken in thesame centre by 2 trained operators. The ozone dose was consistentwith the recommended optimal concentration.25,38In our opinion, scanner guidance is more secure, allowing formeticulous positioning of the needle and, thus, avoiding potentialcomplications.40 In addition, CT permits to avoid intradiscal contrastinjection, which, even at low doses, reduces the discal absorption ofozone.42In contrast to many studies, we did not perform complementaryepidural injections of corticosteroids, which could have resulted inthe overestimation of efficiency in the literature.16,35,42-454.4.2. LimitationsThe small number of patients and treated discs were responsiblefor a lack of statistical power that could explain nonsignificantresults.
6. Wei CJ, Li YH, Chen Y, et al. Percutaneous intradiscal oxygen-ozone injection forlumbar disc herniation: no need of perioperative antibiotic prophylaxis. South MedUniv. 2007;27(3):384–386.7. Muto M, Avella F. Percutaneous treatment of herniated lumbar disc by intradiscaloxygenozone injection. Interv Neuroradiol. 1998;4(4):279–286. https://doi.org/10.1177/159101999800400403.8. Fyllos AH, Arvanitis DL, Karantanas AH, Varitimidis SE, Hantes M, Zibis AH. Magneticresonance morphometry of the adult normal lumbar intervertebral space.Surg Radiol Anat. 2018;40(9):1055–1061. https://doi.org/10.1007/s00276-018-2048-7.9. Modic MT, Steinberg PM, Ross JS, Masaryk TJ, Carter JR. Degenerative disk disease:assessment of changes in vertebral body marrow with MR Imaging. Radiology.1988;1:193–199. https://doi.org/10.1148/radiology.166.1.3336678.10. Pfirrmann CW, Metzdorf A, Zanetti M, Hodler J, Boos N. Magnetic resonance classificationof lumbar intervertebral disc degeneration. Spine. 2001;26(17):1873–1878.https://doi.org/10.1097/00007632-200109010-00011.11. Lam KS, Carlin D, Mulholland RC. Lumbar disc high-intensity zone: the value andsignificance of provocative discography in the determination of the discogenic painsource. Eur Spine J. 2000;9(1):36–41. https://doi.org/10.1007/s005860050006.12. Vanni D, Galzio R, Kazakova A, et al. Intraforaminal ozone therapy and particularside effects: preliminary results and early warning. Acta Neurochir. 2016;158(3):491–496. https://doi.org/10.1007/s00701-015-2545-y.13. Steppan J, Meaders T, Muto M, Murphy KJ. A metaanalysis of the effectiveness andsafety of ozone treatments for herniated lumbar discs. J Vasc Interv Radiol. 2010;21(4):534–548. https://doi.org/10.1016/j.jvir.2009.12.393.14. Ercalik T, Kilic M. Efficacy of intradiscal ozone therapy with or without periforaminalsteroid injection on lumbar disc herniation: a double-blinded controlled study.Pain Physician. 2020;23(5):477–484.15. Crockett MT, Moynagh M, Long N, et al. Ozone-augmented percutaneous discectomy:a novel treatment option for refractory discogenic sciatica. Clin Radiol.2014;69(12):1280–1286. https://doi.org/10.1016/j.crad.2014.08.008.16. Ezeldin M, Leonardi M, Princiotta C, et al. Percutaneous ozone nucleolysis for lumbardisc herniation. Neuroradiology. 2018;60(11):1231–1241. https://doi.org/10.1007/s00234-018-2083-4.17. Schenk B, Brouwer PA, Peul WC, van Buchem MA. Percutaneous laser disk decompression:a review of the literature. Am J Neuroradiol. 2006;27(1):232–235.18. Klessinger S. The frequency of resurgery after lumbar disc Nucleoplasty in a tenyearperiod. Clin Neurol Neurosurg. 2018;170:79–83. https://doi.org/10.1016/j.clineuro.2018.05.004.19. Runge M. La chimionucl eolyse. Ann Kin esith er Masson Paris. 1987:431–437.20. Andr es-Cano P, Vela T, Cano C, García G, Vera JC, Andr es-García JA. Cervical spondylodiscitisafter oxygen-ozone therapy for treatment of a cervical disc herniation:a case report and review of the literature. HSS J. 2016;12(3):278–283. https://doi.org/10.1007/s11420-016-9500-1.21. Bo W, Longyi C, Jian T, et al. A pyogenic discitis at c3-c4 with associated ventral epiduralabscess involving c1-c4 after intradiscal oxygen-ozone chemonucleolysis: a case report.Spine. 2009;34(8):298–304. https://doi.org/10.1097/BRS.0b013e318195a87e.22.22. Yang CS, Zhang LJ, Sun ZH, Yang L, Shi FD. Acute prevertebral abscess secondaryto intradiscal oxygen-ozone chemonucleolysis for treatment of a cervicaldisc herniation. J Int Med Res. 2018;46(6):2461–2465. https://doi.org/10.1177/ 0300060518764186.23. Lehnert T, Naguib NN, Wutzler S, et al. Analysis of disk volume before and after CTguidedintradiscal and periganglionic ozone-oxygen injection for the treatment oflumbar disk herniation. J Vasc Interv Radiol. 2012;23(11):1430–1436. https://doi.org/10.1016/j.jvir.2012.07.029.24. Bonetti M, Zambello A, Leonardi M. Princiotta. Herniated disks unchanged overtime: size reduced after oxygen-ozone therapy. Interv Neuroradiol. 2016;22(4):466–472. https://doi.org/10.1177/1591019916637356.25. Elawamy A, Kamel EZ, Hassanien M, Wahba OM, Amin SE. Implication of two differentdoses of intradiscal ozone-oxygen injection upon the pain alleviation inpatients with low back pain: a randomized, single-blind study. Pain Physician.2018;21(1):25–31.26. Bruno F, Smaldone F, Varrassi M, et al. MRI findings in lumbar spine following O2-O3 chemiodiscolysis: a long-term follow-up. Interv Neuroradiol. 2017;23(4):444–450. https://doi.org/10.1177/1591019917703784.
Two patients received oxygen-ozone injections at 2 different levelsduring the same procedure. The effectiveness of the treatmentwas not differentiable from one level to another, and we had to takethis into account in our statistical analysis.5. ConclusionIn conclusion, our preliminary findings show that oxygen-ozonetherapy in disc herniation realized under CT-scan guidance is safeand effective when conservative treatment and epidural or facet jointsteroid injection failed to relief pain.O2-O3 therapy improves pain in most patients.Based on your first results, we wonder whether this treatmentshould be reserved for patients with nerve root symptoms, ratherthan for those with only low back pain. We assume that the effectivenessof the treatment is both mechanical, related to a decrease in thepressure of the disc on the nerve root, whatever the location of thehernia, and chemical, linked to the anti-inflammatory properties ofozone.Furthermore, we suggest that the presence of low calcifications inthe disc herniation should not be a contraindication.This treatment had no impact on any future spine surgery.Intra-discal oxygen-ozone therapy is an easy and low cost procedurebut it’s not widely used in France.These promising preliminary results have convinced us of the usefulnessand the safety of this treatment, and we hope that it will bemore wildly used in our country.Funding sourcesThis research did not receive any specific grant from fundingagencies in the public, commercial, or not-for-profit sectors.Declaration of Competing InterestThe authors declare that they have no competing interest.CRediT authorship contribution statementCl ementine Simon: Investigation, Data curation, Writing − originaldraft. Thomas Le Corroller: Methodology, Data curation. VanessaPauly: Conceptualization, Supervision. Daphne Guenoun: Conceptualization,Methodology, Validation, Writing − review & editing,Supervision.AcknowledgementThe authors thank the Assistance Publique des H^opitaux de Marseille(APHM).Supplementary materialsSupplementary material associated with this article can be foundin the online version at doi:10.1016/j.neurad.2021.09.004.References1. Balagu e F, Mannion AF, Pellis e F, Cedraschi C. Non-specific low back pain. Lancet.2012;379(9814):482–491. https://doi.org/10.1016/S0140-6736(11)60610-7.2. Hashemi M, Poorfarokh M, Mohajerani SA, et al. Injection of intradiscal O2-O3 toreduce pain and disability of patients with low back pain due to prolapsed lumbardisk. Anesth Pain Med. 2014;4(5):e19206. https://doi.org/10.5812/aapm.19206.3. Crock HV. Observations on the management of failed spinal operations. Bone JtSurg. 1976;58−B:193–199.4. De S eze M, Cugy E, Bassiri A. Traitements percutan es intra-discaux dans les lombosciatiqueset les lombalgies. Rev du Rhum Monogr. 2013;80(4):247–251.5. Costa T, Linhares D, Ribeiro da Silva M, Neves N. Ozone therapy for low back pain. Asystematic review. Acta Reumatol Port. 2018;43(3):172–181.
27. Splendiani A, Perri M, Conchiglia A, et al. MR assessment of lumbar disk herniationtreated with oxygen-ozone diskolysis: the role of DWI and related ADC versusintervertebral disk volumetric analysis for detecting treatment response. NeuroradiolJ. 2013;26(3):347–356. https://doi.org/10.1177/197140091302600316.28. Buric J, Rigobello L, Hooper D. Five and ten year follow-up on intradiscal ozoneinjection for disc herniation. Int J Spine Surg. 2014;8:17. https://doi.org/10.14444/1017.29. Apuzzo D, Giotti C, Pasqualetti P, Ferrazza P, Soldati P, Zucco GM. An observationalretrospective/horizontal study to compare oxygen-ozone therapy and/or globalpostural re- education in complicated chronic low back pain. Funct Neurol.2014;29(1):31–39.30. Lee JS, Hobden E, Stiell IG, Wells GA. Clinically important change in the visual analogscale after adequate pain control. Acad Emerg Med. 2003;10(10):1128–1130.https://doi.org/10.1111/j.1553-2712.2003.tb00586.x.31. Muto M, Giurazza F, Silva RP, Guarnieri G. Rational approach, technique andselection criteria treating lumbar disk herniations by oxygen-ozone therapy.Interv Neuroradiol. 2016;22(6):736–740. https://doi.org/10.1111/j.1553-2712.2003.tb00586.x.32. Lutze M, Stendel R, Vesper J, Brock M. Periradicular therapy in lumbar radicularsyndromes: methodology and results. Acta Neurochir. 1997;139(8):719–724.https://doi.org/10.1007/BF01420044.33. Bryce DA, Nelson J, Glurich I, Berg RL. Intradiscal electrothermal annuloplasty therapy:a case series study leading to new considerations. WMJ. 2005;104(6):39–46.34. Oder B, Loewe M, Reisegger M, Lang W, Ilias W, Thurnher SA. CT-guided ozone/steroidtherapy for the treatment of degenerative spinal disease - Effect of age, gender,disc pathology and multi-segmental changes. Neuroradiology. 2008;50(9):777–785. https://doi.org/10.1007/s00234-008-0398-2.35. Enthoven P, Skargren E, Carstensen J, Oberg B. Predictive factors for 1-year and 5-year outcome for disability in a working population of patients with low back paintreated in primary care. Pain. 2006;122(1−2):137–144. https://doi.org/10.1016/j.pain.2006.01.022.36. Alcouffe J, Manillier P, Brehier M, Fabin C, Faupin F. Analysis by sex of low backpain among workers from small companies in the Paris area: severity and occupationalconsequences. Occup Environ Med. 1999;56(10):696–701. https://doi.org/10.1136/oem.56.10.696.37. Perri M, Marsecano C, Varrassi M, Giordano AV, Splendiani A, di Cesare E. Indicationsand efficacy of O2-O3 intradiscal versus steroid intraforaminal injection in differenttypes of disco vertebral pathologies: a prospective randomized double blindtrial with 517 patients. Radiol Medica. 2016;121(6):463–471. https://doi.org/10.1007/s11547-015-0598-x.38. Muto M, Andreula C, Leonardi M. Treatment of herniated lumbar disc by intradiscaland intraforaminal oxygen-ozone (O2-O3) injection. J Neuroradiol. 2004;31:183–189. https://doi.org/10.1016/s0150-9861(04)96989-1.39. Ghatge S, Modi PD, Modi DB. Clinical and radiological improvement followingozone disc nucleolysis: a case report. Cureus. 2017;9(4):e1162. https://doi.org/10.7759/cureus.1162.40. Amoretti N, Hauger O, Marcy PY, Amoretti ME, Lesbats V, Yvonne M. Percutaneousdiscectomy on lumbar radiculopathy related to disk herniation: why under CTguidance? An open study of 100 consecutive patients. Eur J Radiol. 2012;81(6):1259–1264. https://doi.org/10.1016/j.ejrad.2011.02.071.41.41. Lu W, Li Y-H, He X-F. Treatment of large lumbar disc herniation with percutaneousozone injection via the posterior-lateral route and inner margin of the facet joint.World J Radiol. 2010;2(3):109–112. https://doi.org/10.4329/wjr.v2.i3.109.42. Andreula C. Ozone therapy. Neuroradiology. 2011;53(S1):207–209. https://doi.org/10.1007/s00234-011-0930-7.43.43. Perri M, Grattacaso G, Di Tunno V, Marsecano C, Di Cesare E, Splendiani A.MRI DWI/ADC signal predicts shrinkage of lumbar disc herniation after O2-O3discolysis. Neuroradiol J. 2015;28(2):198–204. https://doi.org/10.1177/1971400915576658.44. Gallucci M, Limbucci N, Zugaro L, et al. Sciatica: treatment with intradiscal andintraforaminal injections of steroid and oxygen-ozone versus steroid only. Radiology.2007;242(3):907–913. https://doi.org/10.1148/radiol.2423051934.45. Zhang Y, Ma Y, Jiang J, Ding T, Wang J. Treatment of the lumbar disc herniationwith intradiscal and intraforaminal injection of oxygen-ozone. J Back MusculoskeletRehabil. 2013;26(3):317–322. https://doi.org/10.3233/BMR-130386.